RGMa Inhibition for Repair and Protection in Multiple Sclerosis
Patients with MS have an urgent need for therapies that can reverse neurologic disability by promoting remyelination, and RGMa inhibition may help meet that need.


Multiple sclerosis (MS) is an autoimmune-mediated disorder of the central nervous system (CNS). There is currently no single defined cause of MS development, but the neurological impairments characteristic of the disease are thought to result from auto-immune- or inflammation-mediated axonal demyelination that impedes nerve conduction.1 Drug development for MS has been challenging, in part because a comprehensive treatment should address effects of the disease on both the immune system and CNS. Available treatments, which are largely immunosuppressive, cannot reverse neurological deficits by stimulating remyelination or halting progressive neuronal dysfunction. Thus, concurrent treatment of autoimmune reactions and axonal degeneration has been proposed as a potentially more effective approach to MS therapy.1


Jennifer S. Sun, PhD

Repulsive guidance molecule-a (RGMa) is a glycosylphosphatidylinositol-anchored membrane protein that, upon binding its receptor neogenin, inhibits neuronal regeneration and regulates cell death.1-3 Expression of RGMa is upregulated in the CNS of patients with MS, where RGMa is found in active and chronic lesions, normal-appearing gray and white matter, and meningeal infiltrates.2 In MS, RGMa enhances activation of CD4-positive T cells by dendritic cells presenting myelin sheath self-antigens, initiating an autoimmune response in the white matter of the brain and spinal cord and resulting in axonal demyelination, neurodegeneration, and progressive paralysis.1-3 The multiple functions of RGMa in the CNS and immune system offer an opportunity to therapeutically and concurrently block the autoimmune reactions and axonal injury observed in neurodegenerative and neuroinflammatory diseases.
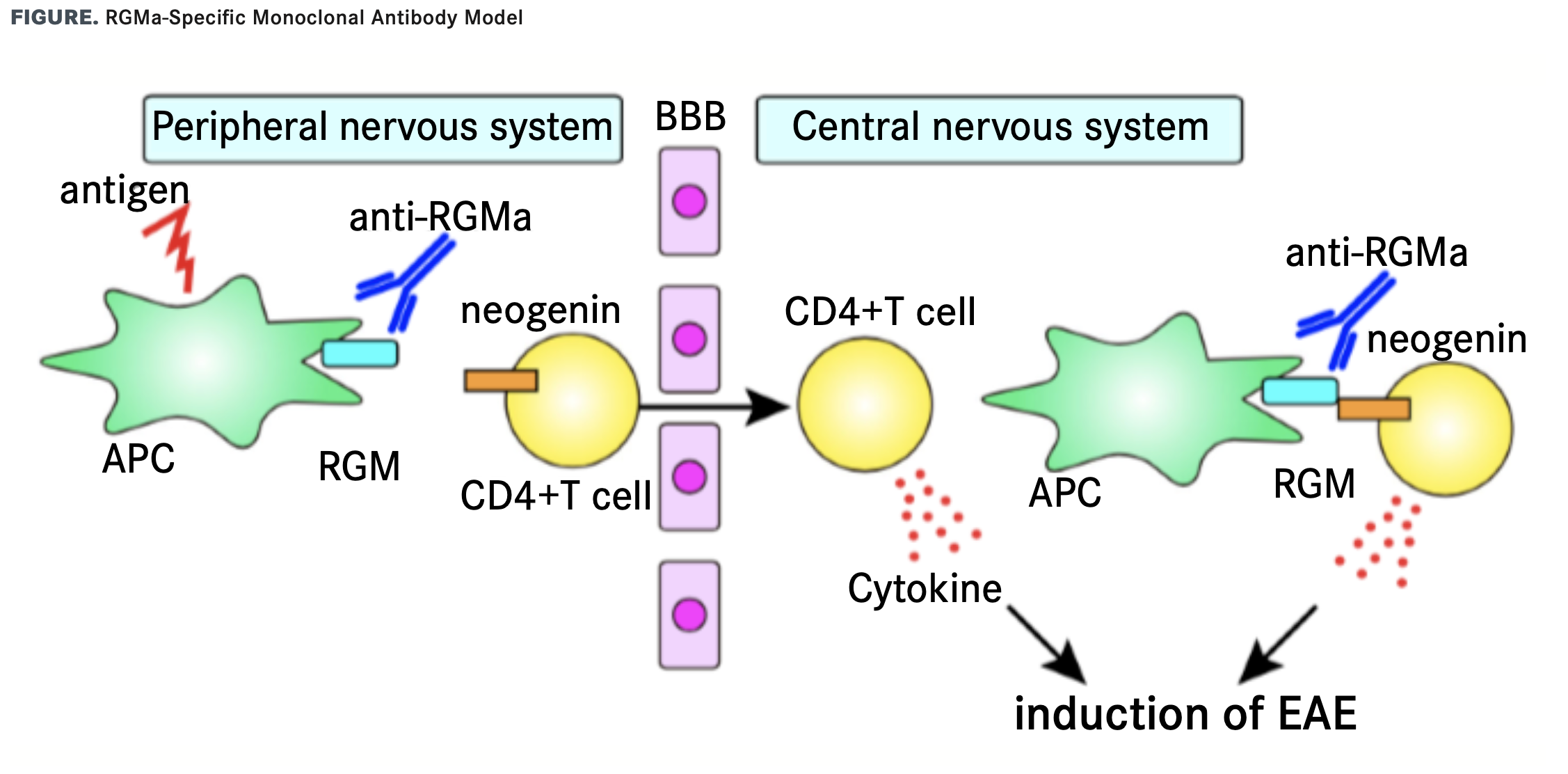
Patients with MS have an urgent need for therapies that can reverse neurologic disability by promoting remyelination.4 RGMa- specific monoclonal antibody (mAb) treatment (FIGURE) promises to surpass the current standard of care for MS, which primarily relies on disease-modifying therapies and symptom management. Anti-RGMa mAbs have been shown to attenuate the severity of animal models of MS, such as experimental autoimmune encephalomyelitis (EAE), by inhibiting T-cell activation in the CNS3,5 while promoting neuroprotection and neuroregeneration.1,2,6 Along with decreased expression of RGMa in the spinal cord, EAE mouse survival was prolonged, accompanied by suppressed secondary progression of disease.6 In a rat model of spinal cord injury, the beneficial effects of anti-RGMa mAb administration were observed over a period of up to 24 hours post-injury. These benefits included reduced tissue degeneration and promotion of neuronal sparing, axonal plasticity, and functional recovery.7

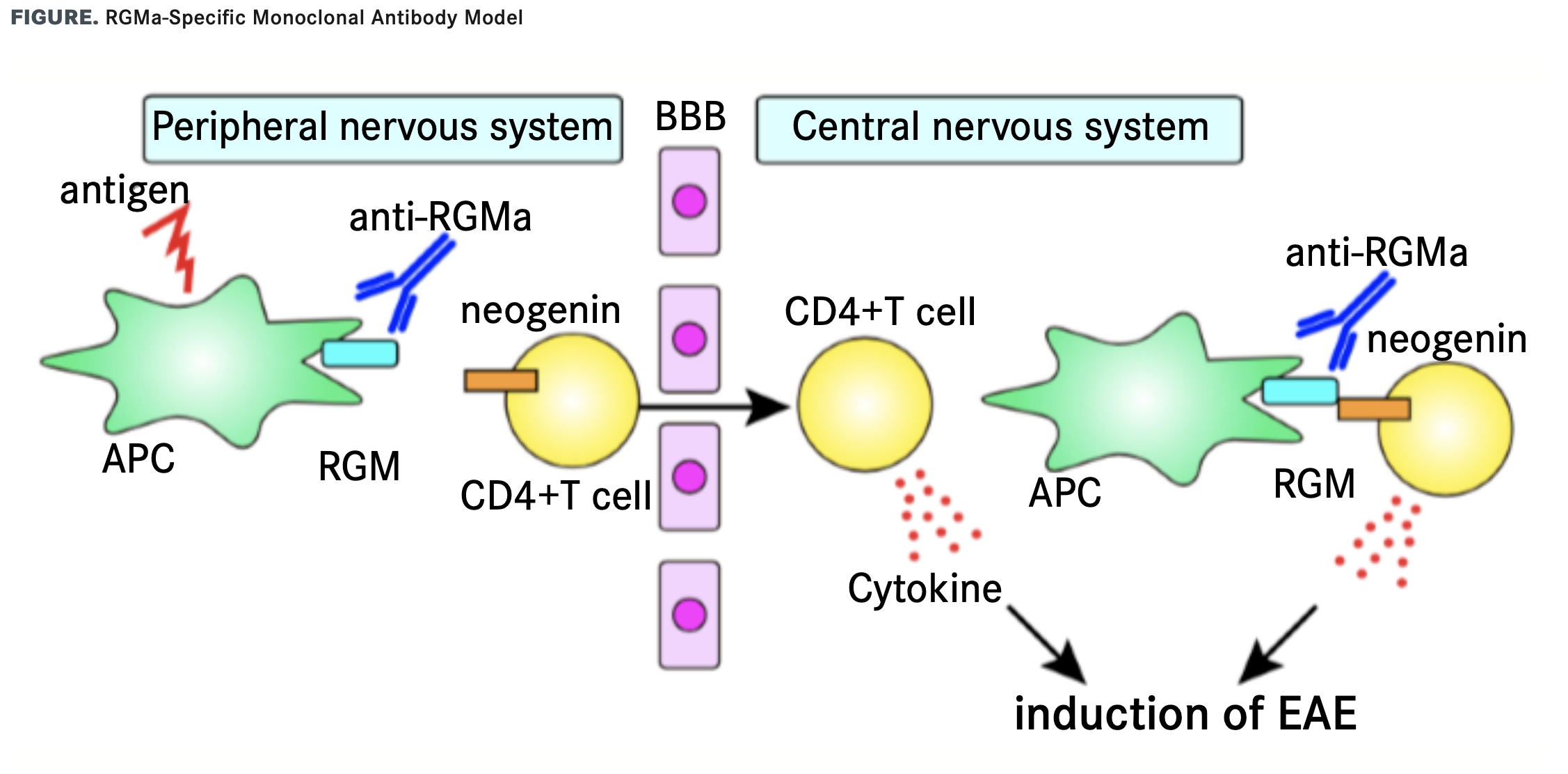
RGMa-neogenin signaling mediates experimental autoimmune encephalomyelitis (EAE), an animal model of multiple sclerosis. Blocking RGMa activity with a neutralizing antibody diminishes immune responses in both the peripheral and central nervous systems. AAPC, antigen-presenting cell; BBB, blood-brain barrier; EAE, experimental autoimmune encephalomyelitis; RGM, repulsive guidance molecule. Reprinted with permission from Fujita and Yamashita. Inflamm Regen. 2017; 37(1):6. doi:10.1186/s41232-017-0037-6
Elezanumab (ABT-555; AbbVie) is a fully-humanized anti-RGMa mAb that has demonstrated promotion of axonal regeneration, neuroprotection, remyelination, and immune modulation in MS-relevant preclinical models. A phase 1, double-blind, placebo-controlled, randomized, escalating 4-dose 29-week study was completed in April 2018 (NCT02601885). The study examined 3 treatment groups (150 mg, 600 mg, and 1800 mg elezanumab via intravenous infusion) and 1 placebo group to determine safety and tolerability in 20 patients with relapsing forms of MS.8 Adverse events (AEs), cerebrospinal fluid (CSF) and plasma biomarker analyses, and Expanded Disability Status Scale (EDSS) scores were assessed. Increasing levels of elezanumab were associated with decreased free soluble RGMa and increased interleukin-10 in CSF. EDSS scores were unchanged. Overall, elezanumab was well tolerated, with the most common AE being headache, and treatment did not consistently result in symptom worsening in patients who received multiple doses up to 1800 mg.8
Elezanumab was granted orphan drug and fast track designations by the FDA on September 28, 2020, for treatment of spinal cord injuries.9 Two long-term, phase 2 studies are underway to elucidate the efficacy of elezanumab in larger patient populations. The RADIUS-R trial (NCT03737851), which commenced in December 2018, enrolled 208 participants with relapsing forms of MS. The RADIUS-P trial (NCT03737812), which began in February 2019, enrolled 123 participants with progressive forms of MS. Both randomized, double-blind, placebo-controlled, multiple-dose studies are assessing the safety and efficacy of elezanumab when added to standard of care and have an estimated study completion date of October 2021. In both trials, patients are randomly assigned to receive 1 of 2 doses of either elezanumab or placebo by intravenous infusion every 4 weeks for 48 weeks. Improvement in measures of physical disability (EDSS, Timed 25-Foot Walk, and 9-Hole Peg Test scores) is recorded at week 52 as the primary outcome.10
Therapeutic antibodies are especially effective for diseases with clearly elucidated molecular mechanisms for which the specific molecules involved in pathogenesis have been identified. Despite its demonstrated efficacy, anti-RGMa mAb therapy does not address some aspects of MS progression, suggesting complexities in the mechanisms of this disease that may not be fully dependent on RGMa. The MS therapeutics market currently has multiple late-stage pipeline products with diverse mechanisms of action (eg, antioxidants; the mAb opicinumab, which inhibits LINGO-1, a negative regulator of axonal myelination11; and sodium channel blockers12). RGMc-based therapy is also a promising avenue worth exploring. RGMc, a member of the RGM family whose expression is limited to striated muscle and the liver, is downregulated in the sera of mice induced with EAE.13,14 Treatment with soluble RGMc enhanced the integrity of the blood-brain barrier to significantly delay the onset of EAE and reduce its clinical severity.13 Overall, with each new intervention undergoing development, investigators will gain further insight into the disease process of MS and eventually pinpoint the key molecular drivers of this disease.
For correspondence: jssun@princeton.edu
REFERENCES
1. Kubo T, Tokita S, Yamashita T. Repulsive guidance molecule-a and demyelination: implications for multiple sclerosis. J Neuroimmune Pharmacol. 2012;7(3):524-528. doi:10.1007/s11481-011-9334-z 2. Demicheva E, Cui Y-F, Bardwell P, et al. Targeting repulsive guidance molecule a to promote regeneration and neuroprotection in multiple sclerosis. Cell Rep. 2015;10(11):1887-1898. doi:10.1016/j.celrep.2015.02.048
3. Muramatsu R, Kubo T, Mori M, et al. RGMa modulates T cell responses and is involved in autoimmune encephalomyelitis. Nat Med. 2011;17(4):488-494. doi:10.1038/nm.2321
4. Göttle P, Förster M, Weyers V, et al. An unmet clinical need: roads to remyelination in MS. Neurol Res Pract. 2019;1(1):21. doi:10.1186/s42466-019-0026-0
5. Harada K, Fujita Y, Okuno T, et al. Inhibition of RGMa alleviates symptoms in a rat model of neuromyelitis optica. Sci Rep. 2018;8. doi:10.1038/s41598-017-18362-2
6. Tanabe S, Fujita Y, Ikuma K, Yamashita T. Inhibiting repulsive guidance molecule-a suppresses secondary progression in mouse models of multiple sclerosis. Cell Death Dis. 2018;9(11). doi:10.1038/s41419-018-1118-4
7. Mothe AJ, Coelho M, Huang L, et al. Delayed administration of the human anti-RGMa monoclonal anti-body elezanumab promotes functional recovery including spontaneous voiding after spinal cord injury in rats. Neurobiol Dis. 2020;143:104995. doi:10.1016/j.nbd.2020.104995
8. Ziemann A, Rosebraugh M, Barger B, Cree B. A phase 1, multiple-dose study of elezanumab (ABT-555) in patients with relapsing forms of multiple sclerosis (S56.001). Neurology. 2019;92(15 Supplement):S56.001.
9. AbbVie receives orphan drug and fast track designations from the U.S. Food and Drug Administration for elezanumab, an investigational monoclonal antibody RGMa inhibitor, for the treatment of spinal cord injury. News release. Abbvie. September 28, 2020. Accessed October 30, 2020. https://www.biospace. com/article/releases/abbvie-receives-orphan-drug-and-fast-track-designations-from-the-u-s-food- and-drug-administration-for-elezanumab-an-investigational-monoclonal-antibody-rgma-inhibitor-for- the-treatment-of-spinal-cord-injury/
10. Cree B, Pfleeger K, Schwefel B, Ziemann A. Investigating the safety and efficacy of elezanumab in two phase 2 studies enrolling patients with different disease courses of multiple sclerosis (1219). Neurology. 2020;94(15 Supplement). Accessed October 27, 2020. https://n.neurology.org/ content/94/15_Supplement/1219
11. Cadavid D, Balcer L, Galetta S, et al; RENEW Study Investigators. Safety and efficacy of opicinumab in acute optic neuritis (RENEW): a randomised, placebo-controlled, phase 2 trial. Lancet Neurol. 2017;16(3):189-199. doi:10.1016/S1474-4422(16)30377-5
12. Raftopoulos R, Hickman SJ, Toosy A, et al. Phenytoin for neuroprotection in patients with acute optic neuritis: a randomised, placebo-controlled, phase 2 trial. Lancet Neurol. 2016;15(3):259-269. doi:10.1016/ S1474-4422(16)00004-1
13. Kuns-Hashimoto R, Kuninger D, Nili M, Rotwein P. Selective binding of RGMc/hemojuvelin, a key protein in systemic iron metabolism, to BMP-2 and neogenin. Am J Physiol-Cell Physiol. 2008;294(4):C994-C1003. doi:10.1152/ajpcell.00563.2007
14. Vigouroux RJ. Identifying the role of RGMc in an animal model of Multiple Sclerosis. [master’s thesis]. Toronto, Ontario, Canada: University of Toronto. 2015.